| Type of paper: | Essay |
| Categories: | Gender Health and Social Care Research |
| Pages: | 10 |
| Wordcount: | 2622 words |
Demographics research
This section depicts the results gathered from the research. Different results were recorded depending on the demographics. Some of the results have been illustrated in tables and graphs so that the results can be visualized better. Moreover, the mean of every demographic was gathered then carefully analyzed. The results from the demographic will be looked at separately; this entails the age, gender, referral location and diagnosis. This will be concurrently compared with the related literature.

All the data that was collected from the patients was appropriately divided and the results adequately organized. Patients with just one HbA1c value were eliminated because they lacked information that could be assessed by comparing it with their glycemic control. The results from every demographic group will be averaged out.
Gender distribution
The study included 297 females and 305 males; a total of 602 patients were selected. Collectively, the males constituted for 50.6 percent of the research group while the women represented 49.3 percent. It is important to note that Hba1c was found to be in higher levels in men as compared to the women. There was a study carried out on Caucasian patients that examined gender equality in the management of HbA1c and it found that there was no result difference between the male and female patients with regards to the glycemic levels. However, the study concluded that women usually have lower glycemic results probably due to hormonal changes, pregnancy, lifestyle (e.g. dieting), and social factors.
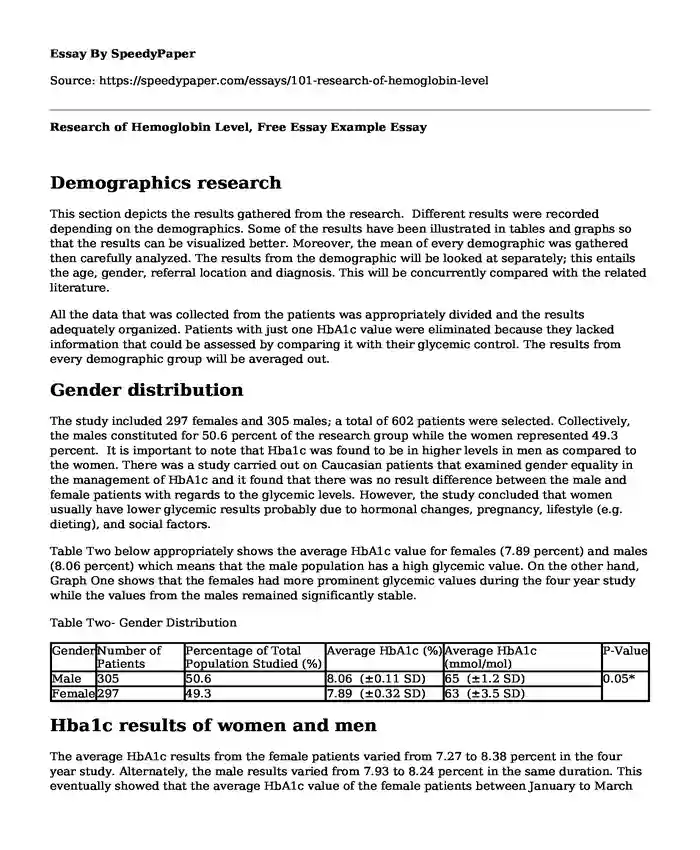
Table Two below appropriately shows the average HbA1c value for females (7.89 percent) and males (8.06 percent) which means that the male population has a high glycemic value. On the other hand, Graph One shows that the females had more prominent glycemic values during the four year study while the values from the males remained significantly stable.
Table Two- Gender Distribution
| Gender | Number of Patients | Percentage of Total Population Studied (%) | Average HbA1c (%) | Average HbA1c (mmol/mol) | P-Value |
| Male | 305 | 50.6 | 8.06 (±0.11 SD) | 65 (±1.2 SD) | 0.05* |
| Female | 297 | 49.3 | 7.89 (±0.32 SD) | 63 (±3.5 SD) |
Hba1c results of women and men
The average HbA1c results from the female patients varied from 7.27 to 8.38 percent in the four year study. Alternately, the male results varied from 7.93 to 8.24 percent in the same duration. This eventually showed that the average HbA1c value of the female patients between January to March was a bit higher as compared to the men. In fact, the female patients began with the average of 8.38 percent with regards to the HbA1c value while the men began with 8.20 percent.
It is evident that this result is similar to most of the studies highlighted in the literature review meaning that the hypoglycemic levels are normally higher in women. However, this depends on the lifestyle activities of the gender. The women experience hormonal changes and pregnancy and this influences their behavioral aspects and lifestyles which makes them stand out from the men. Furthermore, cultural differences have been blamed for this difference mainly because the men are believed to be more active as compared to the women depending on the shaping of the society.36 Women may attend more gatherings that have desserts and food as compared to the men and this diet difference may be the cause of this results.42
The graph on the other hand shows an unstable tendency from the females whereby the HbA1c apparently decreases and increases. The female curve started at 8.38 percent and stopped at 7.69 percent; this is a falling curve. This means that the female patients reduced their glycemic values irrespective of the value fluctuation within the three year period of data collection. Hence, the HbA1c values went down by 0.69 percent. The male curve shows that the HbA1c results reduce from 8.20 percent to 8.07 percent (0.1 percent difference) which is a significant difference with regards to the male glycemic levels.
The reason why males have a higher glycemic value as compared to the women is due to the fact that women have estrogen that protects the β-cell functions and this stops the development of insulin resistivity as well as diabetes. Furthermore, females usually go through menopause and this triggers estrogen replacement which promotes insulin sensitivity. Moreover, it has been proven that certain female hormones such as sex hormones contribute positively to insulin sensitivity.52
Age groups HbA1c results
The age category included six hundred participants; two hundred and fifty three were eliminated because they lacked sufficient information to examine the HbA1c results. This analysis needed more than a single HbA1c value during the entire three year duration so that it could be included in the comparisons.
The ages were distributed in ten year sequences per group. Most of the patients were placed in the 51 to 60 year old age group which included 201patients; this is roughly equivalent to 33 percent of the research population. The second largest group was the 41 to 50 year old patients that represented 160 patients; equal to 26 percent of the patients. The rest of the age group classifications and percentages are represented in Table Three below.
Table Three- Age Summary
| Age Groups (Years) | Number of Patients | Percentage of Total Population Studied (%) | Average HbA1c (%) | Average HbA1c (mmol/mol) |
| 0-10 | 1 | 0.17 | 14.68 (±0.69 SD) | 136 (±7.5 SD) |
| 11-20 | 11 | 1.83 | 8.66 (±0.74 SD) | 71 (±8.1 SD) |
| 21-30 | 12 | 1.99 | 7.96 (±0.86 SD) | 63 (±9.4 SD) |
| 31-40 | 41 | 6.82 | 7.73 (±0.69 SD) | 61 (±7.5 SD) |
| 41-50 | 160 | 26.62 | 8.11 (±0.33 SD) | 65 (±3.6 SD) |
Evidently, the younger patients show that the HbA1c levels go up which may be translated to mean that the younger patients are more insulin resistant as compared to older patients. Therefore, older patients do not have the ability to maintain the normal glycemic levels. The 81 to 90-year-old patients (7.52% ±0.41) faced the most noteworthy differences when compared with all the other age groups. A significant difference was computed with their age group compared to the 11-20 years old (8.66% ±0.74), p=0.01, where the 81 to 90-year-old patients experienced lower glycemic values. When being compared to the 41 to 50-year-old age group (8.11% ±0.33), the 81-90 aged patient had significantly lower glycemic levels, p=0.01.
Patients’ HbA1c results in Referral Location
The sum of the various patients’ HbA1c results was averaged out, the mean obtained and recorded. In total, five hundred and ninety seven patients from forty five locations were entailed in this section. The patients came from various poly clinics, inpatient wards and outpatient clinics. After entering the patient information, patients with more than one HbA1c test done, and patients with a referral location written on the request were used in this study. This resulted in a total of two hundred fifty-seven patients being excluded from the study. The remaining patients omitted were unfit to process because not enough information is achieved to either categorize them (if referral location was missing), or if only one HbA1c result was present because it will lead to an inconclusive comparison.
The locations were furthermore combined into three groups:
1. Inpatient
2. Outpatient (within the hospital)
3. Clinic (polyclinics in various cities)
A study found that patients that live within particular locations experience increased hypoglycemic episodes while in the Intensive Care Unit of a hospital because of the procedures they are submitted to throughout their stay. Notably, patients that are dangerously ill could have glycemic levels that are better managed due to the fact that they are keenly monitored by the medical practitioners. These changes in the glycemic levels with regards to the location could be because of a patient’s condition. Hence, if a patient is in critical condition, his/her immune system becomes more vulnerable to the fluctuations as well as the glucose controls. Nevertheless, a patient’s condition may influence their glycemic levels immensely.
The outpatient location featured ninety-nine patients from eleven different locations. The inpatient location consisted of 40 patients from 10 various locations. Finally, the clinic location is made up of 458 patients from 24 different locations (Refer to Appendix I for a detailed depiction of each location). The distribution of patients in each category is shown in table five above. The majority of the patients in this study were referred by clinics. The inpatient and outpatient locations combined to make almost a quarter of the study population, while the clinic location made up 76.72% of the population. The inpatient (7.56% ±0.49) is classified to be in the suboptimal range with an HbA1c value falling between 7-8%. The outpatient and the clinic locations (8.04% ±0.99, 8.06% ±0.26 consecutively) however, were classified under the frankly increased range having HbA1c values between 8-10%.
According to afore mentioned observational study, surgical and medical wards (not categorized as intensive care) had revealed increased hyperglycemic values among the patients and inadequate clinical outcomes. Therefore, patients that have been admitted in hospital are more vulnerable to the episodes due to the delicacy of their conditions. Outpatients usually have self-management when it comes to the glycemic levels because they use Continuous Subcutaneous Insulin Infusion therapy making it easier to control or monitor glucose levels. Hence, the patients attending outpatient clinics are more stable; they can take care of themselves without requiring immediate help.
Analysis of patient diagnosis
Patient diagnosis’ were analyzed and combined into fifteen main groups consisting of subgroups. A total of five hundred sixteen patients were included in this study, while three hundred thirty-eight patients were excluded because they either had insufficient clinical data available (not enough HbA1c test results to perform analysis), or they lacked a diagnosis recorded on the request. The largest diagnosis group is the diabetic patients (n=352), which make up 68.5% of all the diagnosis followed by the lab examination group (n=51) which is 9.92% of the total population. The third largest group is the hypertensive patients (n=44), which make up 8.52%.
Usually, HbA1c is measured in every patient whether diabetic or not. Evidently, patients diagnosed with diabetes have a higher glycemic value, but, the ones with hyperlipidemia and hypertension have an increased diabetes mellitus complication. The enhanced glycemic results are usually linked with the reduced neuropathy, nephropathy and retinopathy. Nevertheless, particular conditions may have a negative or positive effect on the HbA1c concentrations. Studies show that iron deficiency anemia enhances the HbA1c values due to the alteration of the hemoglobin’s molecule structure.24 Furthermore, a positive correlation has been found between the HbA1c concentrations as well as the Hb values.
The distribution of the diagnosis groups and subgroups is as follows:
• Lab Examination
o Check Up (7 patients)
o Lab Examination (19 patients)
o General Medical Examination (17 patients)
o Diagnosis Under Investigation (8 patients)
• Diabetes
o Diabetes Mellitus – unspecified (221 patients)
o Type One Diabetes Mellitus (11 patients)
o Type Two Diabetes Mellitus (109 patients)
o Impaired Fasting and Impaired Glucose Tolerance (3 patients)
o Hyperglycemia (3 patients)
o Diabetes Ketoacidosis (1 patient)
• Gastrointestinal
o Gastritis Water Brash (1 patient)
o Irritable Bowel Disease (1 patient)
o Upper Gastrointestinal Bleed (1 patient)
o Haemorrhoids (1 patient)
• Hypercholesterolemia
o Hypercholesterolemia (4 patients)
o Hyperlipidaemia (3 patients)
o Hypothyroidism (3 patients)
o Hypertension (44 patients)
• Cardiology
o Cardiovascular Arrest (3 patients)
o Left Ventricular Failure (2 patients)
o Chest Pain (1 patient)
o Non-Segment Elevation Myocardial Infarction (1 patient)
o Deep Venous Thrombosis (1 patient)
o Acute Coronary Syndrome (4 patients)
o Atrial Fibrillation (2 patients)
o Angiography (2 patients)
o Coronary Artery Bypass Graft Surgery (1 patient)
o Pulmonary Oedema (1 patient)
o Stroke (1 patient)
o Transient Ischemic Attack (1 patient)
• Kidney Disease
o Chronic Kidney Disease (13 patients)
o Chronic Renal Failure (2 patients)
•Bone Pain and Muscle Cramp
o Bone Pain/Muscle Cramp (1 patient)
o Muscle Cramp (1 patient)
o Joint Disorder (1 patient)
• Iron Deficiency Anemia (1 patient)
• Upper Respiratory Tract Infections
o Asthma (1 patient)
o Bronchial Asthma (1 patient)
o Upper Respiratory Tract Infection (1 patient)
o Pharyngitis (1 patient)
o Community Acquired Pneumonia (1 patient)
o Fever (1 patient)
• Weight Issues
o Obesity (2 patients)
o Post Sleeve (2 patients)
• Hepatitis C (1 patient)
• Urinary Tract Infection (3 patients)
• Loss of Consciousness (1 patient)
Diabetes patients in research
It was found the patients with diabetes had the majority of significant differences when compared with other diagnoses. With reference to table five, the most significant differences were noted between laboratory examination (7.33 ±0.54) and diabetes (8.21 ±0.24), p=0.01, where the diabetic patients experienced higher glycemic levels. Hypertensive patients (6.78 ±0.38), had lower glucose levels than diabetic patients, p=0.01. When comparing cardiology (8.33 ±0.73) and hypertension (6.78 ±0.38), there was a significantly higher HbA1c in the cardiology patients, p=0.01. A total of thirteen significant differences were calculated between the various diagnoses.
The gastrointestinal group (7.38 ±0.62) has a noteworthy difference with the cardiology patients (8.33 ±0.73), p=0.01. The gastrointestinal patients have an average glycemic value of 7.38%, while the cardiology patients have a mean HbA1c of 8.33%. This shows the cardiology patients have a significantly higher average HbA1c than the gastrointestinal group.
It is important to note that hemoglobin A1c is a significant indicator for the assessment and diagnosis of particular conditions and diseases like severe hypertension or hypoglycemia. Therefore, this can be utilized to find states of ongoing hyperglycemia because they cannot alter with the short hyperglycemic spikes or hypoglycemic episodes. Moreover, these results show that Type One diabetic patients affect the HbA1c levels depending on the self-efficacy.
The diabetes group had significant variances with five other diagnoses. When compared with the laboratory examination group (7.33 ±0.54), the diabetic patients (8.21 ±0.24) had a significantly higher glycemic level, p=0.01. Furthermore, the diabetic patients (8.21 ±0.24) had significant differences with the gastrointestinal patients (7.38 ±0.62). The gastrointestinal patients experienced lower glycemic values than the diabetic patients, p= 0.01. The following diagnoses had relatively lower glycemic values when compared to diabetic patients, hypertensive patients (6.78% ±0.38) p= 0.01, chronic kidney disease patients (7.54% ±0.67) p=0.01, and the upper respiratory tract infection patients (6.83% ±1.44) p=0.03. Diabetic patients had the highest glycemic value compared to these diagnoses.
Type 2 diabetic patients
In a similar research conducted in the United States Urban African American population type 2 diabetic patients were used and their glycemic values were measured.52 It concluded there was a high prevalence of obesity and poor glycemic control in young patients with diabetes. This is because young patients might have poor adherence to medication and they cannot control their intake of food and this inevitably leads to uncontrolled glycemic levels.
A related study carried out in the Western Pacific that focused on Type Two Diabetic patients who were below eighteen years of age concluded that additional elements like micro-albuminuria and hypertension increased with diabetes prevalence among patients. 64 Based on the nationality of the patient, glycemic values may vary significantly due to the lifestyle and diets of the different geographical locations. Hence, this study has results that have been influenced by the characteristics of the Kuwait nationals.
The diabetic group is the diagnosis with the most patients because these patients have to follow up regularly. This is because they have already been diagnosed with a type of diabetes and need to keep monitoring their glycemic levels from time to time. Therefore, close examination of the diabetic patients shows a monthly HbA1c average is portrayed in graph three above.
It is essential to note that maintaining an HbA1c of less than 7% is important as well as avoiding hypoglycemia (HbA1c of less than 4%). Temporary increases or decreases of blood glucose do not affect HbA1c levels within the last three to four weeks. Apart from hemoglobinopathies and hemoglobin variants, other factors which affect the result of HbA1c analysis are anemia, hemolysis or heavy bleeding. An example of a factor which increases HbA1c is a patient who is iron-deficient14.
Cite this page
Research of Hemoglobin Level, Free Essay Example. (2018, Jul 16). Retrieved from https://speedypaper.net/essays/101-research-of-hemoglobin-level
Request Removal
If you are the original author of this essay and no longer wish to have it published on the SpeedyPaper website, please click below to request its removal:
- Free Essay: A Sociological Perspective on Crime and Gang Violence in American Society
- What Is a Prosecutor - Law Essay Example
- Free Essay on the Impact of the French Revolution and Enlightenment on the Haitian Revolution
- Essay Sample on China-Japan Border Conflict Reflection
- How American Civil War Helped Form the Modern World
- Analysis of Annual Reports Released by Ford Motor Company and General Motors Company - Essay Sample
- Essay Sample on Pharmaceutical Pricing
Popular categories


